Functional Lab Ranges vs Conventional: Why "Normal" Doesn't Mean Well
Functional lab ranges vs conventional — why your "normal" bloodwork could miss early imbalance, and how optimal ranges reveal what standard labs don't.
On this page Read more
- Functional vs Conventional Lab Ranges: The Quick Answer
- What a Lab Reference Range Really Tells You
- "Normal" vs "Optimal": The Distinction That Changes Everything
- Thyroid: Where the Gap Shows Up Most Clearly
- Other Markers Where Functional and Conventional Ranges Diverge
- The Ferritin Story That Makes This Personal
- When Conventional Ranges Are Exactly Right — Because They Are
- How to Use Both Approaches as a Patient
- Key Takeaways
- Frequently Asked Questions
- Here's What to Remember
Reading time: ~9 min | Last reviewed: July 2026
You've probably been there.
Sitting in your primary care doctor's office, a little nervous, waiting on bloodwork you were sure would finally explain why you've felt so off. The nurse pops in, gives you a thumbs-up, and says something like:
"Great news — everything looks normal!"
And you're supposed to feel relieved. Instead, you walk out feeling dismissed.
If that hits close to home, you're not imagining things — and you're not alone. Millions of Americans leave their annual physical with a clean lab report — and a body that clearly didn't get the memo. That disconnect is exactly what understanding functional lab ranges vs conventional ranges is all about.
Here's the thing: this isn't about one approach being right and the other wrong. It's about what a reference range really measures. And why a result inside that range can still be a long way from where your body runs best.
Functional vs Conventional Lab Ranges: The Quick Answer
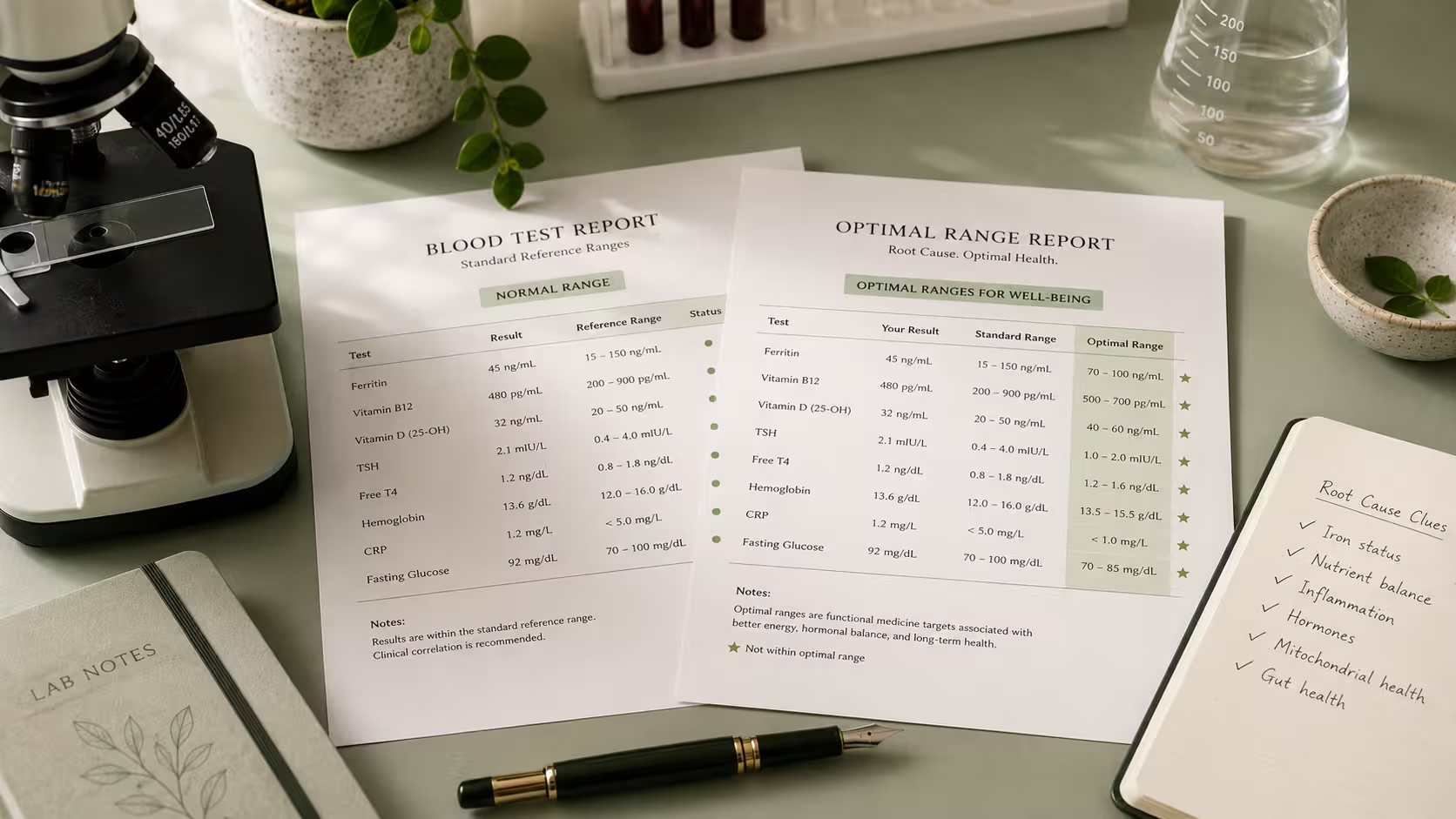
A conventional lab range flags the middle 95% of a tested population as "normal," so it answers one question: is your result common? A functional lab range is narrower and asks a different question: is your result in the band tied to feeling well? A value can read "normal" on a standard panel and still sit outside the optimal range — and that gap is where a lot of unexplained symptoms live.
The rest of this post unpacks how that gap works, where it shows up most, and how to use both frameworks as a patient.
What a Lab Reference Range Really Tells You
Almost no one explains this at the front desk, so let's change that right now.
A conventional lab reference range isn't a map of health. It's a map of a population.
When a lab sets its "normal" range, it draws blood from a large group of people and plots the results. It then flags the middle 95% as the reference interval. Anything inside that window gets a green checkmark. Anything outside gets a little H or L printed in red.
Sounds reasonable — until you look at who's being measured.
That so-called healthy population often isn't especially healthy. It includes people with undiagnosed thyroid issues, early insulin resistance, chronic stress, and low-grade nutrient gaps. When you average a struggling population, you get a range that quietly normalizes the struggle.
That's the heart of the conventional vs functional medicine testing debate. Conventional reference ranges answer: "Is this result statistically common?" Functional reference ranges ask something more useful: "Is this result actually associated with feeling well?"
Those are two very different questions.
"Normal" vs "Optimal": The Distinction That Changes Everything
If you take one idea from this post about normal vs optimal lab values, make it this one.
A "normal" lab value means your result is average. An "optimal" lab value means your result sits in the range tied to real energy, hormonal balance, and feeling like yourself.
They're not the same thing. And the space between them? That's where a lot of unexplained symptoms quietly live.
Picture a number line. At the far ends sit the clearly abnormal results — the territory of serious, diagnosable disease. Conventional medicine is superb at catching those, and that matters. But functional reference ranges narrow the window, zeroing in on the band where research and clinical experience suggest your body actually thrives.
That narrower window is why two people with the same lab printout can get very different answers. One practitioner sees "normal." Another sees a value sitting at the far edge of the range, slowly drifting the wrong way — and links it to the symptoms you've described at every visit.
Neither one is misreading your labs. They're using different functional medicine lab values to read the same number.
Thyroid: Where the Gap Shows Up Most Clearly
Nowhere does the difference between functional and conventional interpretation hit harder than the thyroid.
Conventional thyroid screening often starts — and stops — with one marker: TSH (thyroid-stimulating hormone). The standard range usually runs about 0.5 to 4.5 mIU/L, though it varies by lab. If your TSH comes back at 3.8, most standard panels wave you through with no flags.
Many functional practitioners aim for a tighter optimal window — often cited around 1.0 to 2.0 mIU/L — and they rarely stop at TSH alone. Thyroid lab ranges in functional medicine typically add Free T3, Free T4, Reverse T3, and thyroid antibodies (TPO and TgAb), because those markers reveal how much active thyroid hormone your cells truly receive, and whether your immune system is quietly attacking the gland. (Clinical Endocrinology (via PubMed))
Here's why that matters, in plain terms.
TSH is your brain's way of telling your thyroid to work harder. A normal-but-high TSH can mean your brain is already raising its voice at a gland that's struggling to keep pace. That can happen long before anything crosses the line for a conventional diagnosis. When active thyroid hormone runs low, your cellular metabolism slows. And that slowdown shows up as the exact symptoms people get dismissed for: fatigue, brain fog, cold hands and feet, hair thinning, constipation, low mood, and weight that won't budge. hair loss causes in women
Consider Dana (not her real name), a client in her mid-40s from the Midwest. Her TSH was 3.6 — comfortably inside the normal range. But her Free T3 sat at the very bottom of its window, her Reverse T3 was elevated, and her TPO antibodies were climbing. Standard labs said everything was fine. Functional blood work interpretation told a completely different story — one that matched every symptom she'd been brushed off about for two years. That's thyroid lab ranges in functional medicine doing what a lone TSH cannot.
Other Markers Where Functional and Conventional Ranges Diverge
Thyroid gets the headlines, but it's far from the only place these two frameworks part ways. A few more markers where functional reference ranges tend to run tighter:
- Vitamin D — Standard labs often won't flag a problem until levels drop below 20–30 ng/mL. Many functional practitioners target a higher optimal range for immune support, mood, and bone health.
- Ferritin (iron storage) — A ferritin of 15 is technically within range. But it can sit well below the level needed for steady energy and healthy hair, especially for women who still menstruate. the root cause of low ferritin
- Fasting glucose and hemoglobin A1c — Functional medicine watches for early upward drift in these markers, well before they cross the "prediabetes" cutoff. The goal: catch insulin resistance before it gains traction. (Diabetes Care (via PubMed))
- Vitamin B12 — The low end of the standard range overlaps with levels where some people already have fatigue, brain fog, and early nerve changes. the root cause of morning fatigue
- Homocysteine — A key marker for inflammation and methylation that standard panels often skip entirely.
Notice the pattern. In almost every case, the functional approach is trying to catch a problem earlier — in the window where you feel unwell but haven't yet developed the disease a conventional range is built to catch.
The Ferritin Story That Makes This Personal
Numbers on a page can feel abstract. So let one get specific.
Maya (a composite, not a real person) came in exhausted, losing hair by the handful, and convinced something was wrong — even after years of "everything looks normal." Her ferritin came back at 14. Technically within the reference range. Functionally, a flashing warning light.
Here's the mechanism. Iron is what your body uses to carry oxygen and produce cellular energy. When iron storage falls that low, energy production stalls. And because your body is smart about priorities, it's the high-turnover tissues — like hair follicles — that get cut off first.
Nothing about Maya's labs was abnormal by conventional standards. But by how she felt every single day, every number was a red flag.
That's the whole argument for understanding functional lab ranges vs conventional ones. The goal isn't to manufacture problems that don't exist. It's to stop missing the early, fixable ones.
And honestly? This is exactly why "my labs look normal but I still feel sick" is one of the most-searched health phrases in the US right now. It's one of the most common — and most valid — experiences in modern American healthcare.
When Conventional Ranges Are Exactly Right — Because They Are
Here's where I want to be straight with you, because functional medicine content can overcorrect.
Conventional reference ranges aren't broken. They were built for a specific, critical job: catching serious disease reliably, reproducibly, and at scale across millions of patients. For diagnosing diabetes, flagging kidney trouble, catching severe anemia, or screening for serious disease, those ranges are evidence-based, validated, and life-saving. No functional framework replaces them — and no good functional practitioner would claim otherwise.
Optimal ranges have their own caveats, too. Many rest on clinical experience and new research rather than large controlled trials. And unlike conventional ranges, they're not standardized — so they can vary from one practitioner to the next.
A tighter reference range is a tool for deeper investigation and conversation. It's not a diagnosis.
The most useful way to think about this isn't "conventional bad, functional good." It's both — in sequence. Use conventional ranges to rule out serious disease. Then bring in functional reference ranges as a second lens. Ask whether "not sick" is the same as "thriving" — because for a lot of people, it isn't.
How to Use Both Approaches as a Patient
You don't have to pick a side to benefit from root cause lab testing. Here's a practical path forward:
- Start with standard labs through your primary care doctor. A comprehensive metabolic panel, full thyroid panel, iron studies, vitamin D, and B12 are all reasonable requests. And with most patient portals now, you can pull your own results without waiting for a callback.
- Ask for the actual numbers — not just "normal." That single word hides all the data. Where your result sits within the range matters as much as whether it clears the threshold.
- Track trends, not just single snapshots. A value slowly drifting toward the edge of its range across three annual physicals tells you more than any one result alone.
- Bring both frameworks into the conversation. Root cause lab testing and optimal ranges help you ask sharper questions and push for follow-up when something feels off.
- Work with a qualified practitioner for interpretation. Functional reference ranges are a starting point for a clinical conversation — not a self-diagnosis tool. You want someone who can read the full picture in context.
Key Takeaways
- The core of functional lab ranges vs conventional ranges: "normal" means statistically average, while "optimal" means tied to actually feeling well — not the same thing
- Standard reference ranges come from a population that includes many unwell people, which widens the "normal" window
- Thyroid is where the gap shows up most: conventional care often tests TSH alone, while functional care adds Free T3, Free T4, Reverse T3, and antibodies with tighter targets
- Ferritin, vitamin D, A1c, B12, and homocysteine are other common divergence points — functional ranges catch problems earlier
- Conventional ranges are validated and life-saving for diagnosing disease — functional ranges don't replace them
- Best practice is both, in sequence: rule out disease first, then ask whether "not sick" equals "well"
- Always ask for your actual numbers and track trends across visits
Frequently Asked Questions
What are functional lab ranges, and how are they different from conventional ranges?
Why do functional practitioners say conventional ranges are too broad?
What's the real difference between "normal" and "optimal" lab values?
Which markers are most commonly interpreted differently in functional vs conventional medicine?
Can I use functional lab ranges with my regular doctor?
What does it mean if my labs are normal but I still feel sick?
Here's What to Remember
Remember that exam-room moment — the words that felt like a door quietly closing? "Everything looks normal" was never a lie. It was just an answer to a narrower question than the one you were actually asking.
Conventional ranges tell you whether you're statistically average. Functional ranges ask whether you're genuinely well. The conversation around functional lab ranges vs conventional ones exists because that gap is real. It's measurable, it's meaningful, and it's lived by far too many people who were told there's nothing to investigate.
Your symptoms are data. If your body is signaling something your lab printout doesn't capture, that's not a contradiction to dismiss. It's a clue worth following — with the right tools and the right support on your side.
Wondering how your own numbers stack up? Download the free Optimal Lab Ranges Reference Guide — it maps conventional and functional ranges side by side, so you can walk into your next appointment informed, prepared, and ready to advocate for the care you deserve.
Optimal Lab Ranges Reference Guide
Learn the difference between functional and conventional lab ranges.
Download PDF FreeFact Checked By Dr. Prerana Suryavanshi, MD, MBBS
This medical analysis has been peer-reviewed and vetted by a credentialed practitioner to ensure diagnostic safety.

Written by Dr. Pooja, PharmD
Dr. Pooja didn't set out to write about gut health and hormones. She set out to become a pharmacist — learning how drugs move through the body, why they interact the way they do, and what it actually takes to prove a treatment works. That training is still the lens she writes through today.
View all articles by Dr. Pooja