Case File: 14 Years of "Unexplained" Gut Symptoms — Marcus's GI-MAP Story
For 14 years, Marcus was told his gut was fine. Here's what his GI-MAP test finally found — and why standard testing missed it.
On this page Read more
- The 14-Year Loop: Managed, Never Resolved
- Why "Normal" Results Miss So Much
- What Is a GI-MAP Test, and Why Does It Work Differently?
- Marcus's GI-MAP Results: The Page That Explained 14 Years
- What GI-MAP Results Interpretation Actually Takes
- IBS vs. Gut Infection: Why Your Label Might Not Be the Whole Story
- Is a GI-MAP Test Worth It? An Honest Look
- Key Takeaways
- Frequently Asked Questions
- The Word After "Fine"
Reading time: ~9 min | Last reviewed: July 2026
For 14 years, Marcus was told his gut was "fine."
Fine is a strange word to hear when you've canceled dinners because of bloating. It's stranger still when you've mapped out every bathroom on your commute and watched your energy vanish by 2 p.m. like clockwork. But that's the word that kept coming back — on lab reports, in appointment after appointment, even after a colonoscopy that found "nothing remarkable." Fine.
Marcus isn't his real name. He's a composite of a pattern we see all the time. And he's why this case file exists. When a GI-MAP test finally entered the picture, the thing everyone had missed for over a decade showed up on a single page.
Sound familiar? If you've been handed the word "fine" while your body is telling you something completely different, this one's for you.
(New to this kind of testing? Our complete guide to what the GI-MAP measures and how to read it lives here. This post is the story of what it can uncover in real life.)
The 14-Year Loop: Managed, Never Resolved
Marcus's symptoms didn't show up all at once. They built slowly, the way most gut issues do.
It started in his mid-20s with bloating he blamed on stress and bad takeout. By 30, it was chronic bloating and gas that no amount of "just eat cleaner" advice ever touched. By 35, he'd added loose stools, brain fog, and a fatigue so constant he'd started to assume it was simply what being an adult felt like.
He did everything right. He saw good doctors. He got the full standard workup — a complete blood count, a metabolic panel, a celiac screen, a basic stool test, eventually a colonoscopy. Every result landed within "normal" limits. His doctor called it likely IBS, handed him a fiber pamphlet and a low-FODMAP handout, and sent him on his way.
Here's the trap: IBS is a diagnosis of exclusion. It names what you're experiencing — the symptom pattern — without explaining why. For some people, that's genuinely the end of the story. For Marcus, it meant 14 years of managing symptoms that were never actually traced to their source.
That gap — between "your labs are normal" and "you clearly don't feel normal" — is exactly where so many people get stuck. Let's talk about why it happens.
Why "Normal" Results Miss So Much
Here's something almost nobody tells you: a normal stool test doesn't mean your gut is healthy. It means that particular test didn't find the specific things it looked for, using its particular method.
Conventional stool testing has two real blind spots. First, it relies on culturing organisms in a lab, and plenty of gut microbes are notoriously hard or impossible to grow that way. If an organism doesn't grow, the report never mentions it — even when it's present and actively causing trouble. Second, it screens a short, fixed list of well-known pathogens, because it's built to catch acute infections, not the slow-burn imbalances behind years of chronic symptoms.
Picture searching a house for a gas leak using nothing but your nose. You'd probably catch a big, obvious leak. But a slow, low-level one is different. It's the kind that leaves everyone in the house vaguely unwell for years, and it can slip right past you because your tool isn't sensitive enough.
This is the heart of what functional medicine means by "normal" versus "optimal." They're not the same thing. Standard testing asks, is there an emergency? Gut microbiome testing asks something different: what's actually happening in this ecosystem, and is it working the way it should? functional lab ranges vs. conventional
That reframe — and a GI-MAP test — is what finally moved Marcus's case forward.
What Is a GI-MAP Test, and Why Does It Work Differently?
A GI-MAP test is a comprehensive stool analysis that reads the DNA of the organisms living in your gut.
That one word — DNA — changes everything. The GI-MAP (short for Gastrointestinal Microbial Assay Plus) uses a technology called quantitative PCR, or qPCR. Instead of trying to coax organisms to grow in a dish, it detects and counts their genetic material directly from a single stool sample. If the DNA is there, this functional stool test finds it, whether or not that organism would ever survive a lab culture.
That's what lets it see things a conventional panel structurally can't. A GI-MAP typically reports on:
- Pathogenic bacteria — organisms with a known ability to cause GI illness
- Opportunistic and overgrowth bacteria — normal residents that turn problematic when their numbers spike, the core of gut dysbiosis testing
- H. pylori, including virulence-factor genes that hint at how aggressive a given strain may be — a DNA-based H. pylori stool test can flag this even when other methods come back clean
- Parasites, fungi, and yeast, including species that rarely survive culturing
- Functional markers of digestion (like elastase), inflammation (like calprotectin), and immune activity (like secretory IgA)
That last group matters more than most people realize. The GI-MAP doesn't just ask who's living in there — it asks how well is this gut actually doing its job? You can see, on one page, whether someone is digesting food properly, whether their gut lining is inflamed, and whether their immune system is on high alert.
For someone like Marcus, whose "normal" results never captured any of that, this lens changes everything.
Quick answer: A GI-MAP test is a DNA-based (qPCR) stool test that detects and measures gut bacteria, parasites, fungi, H. pylori, and markers of digestion and inflammation — catching imbalances that culture-based tests routinely miss.
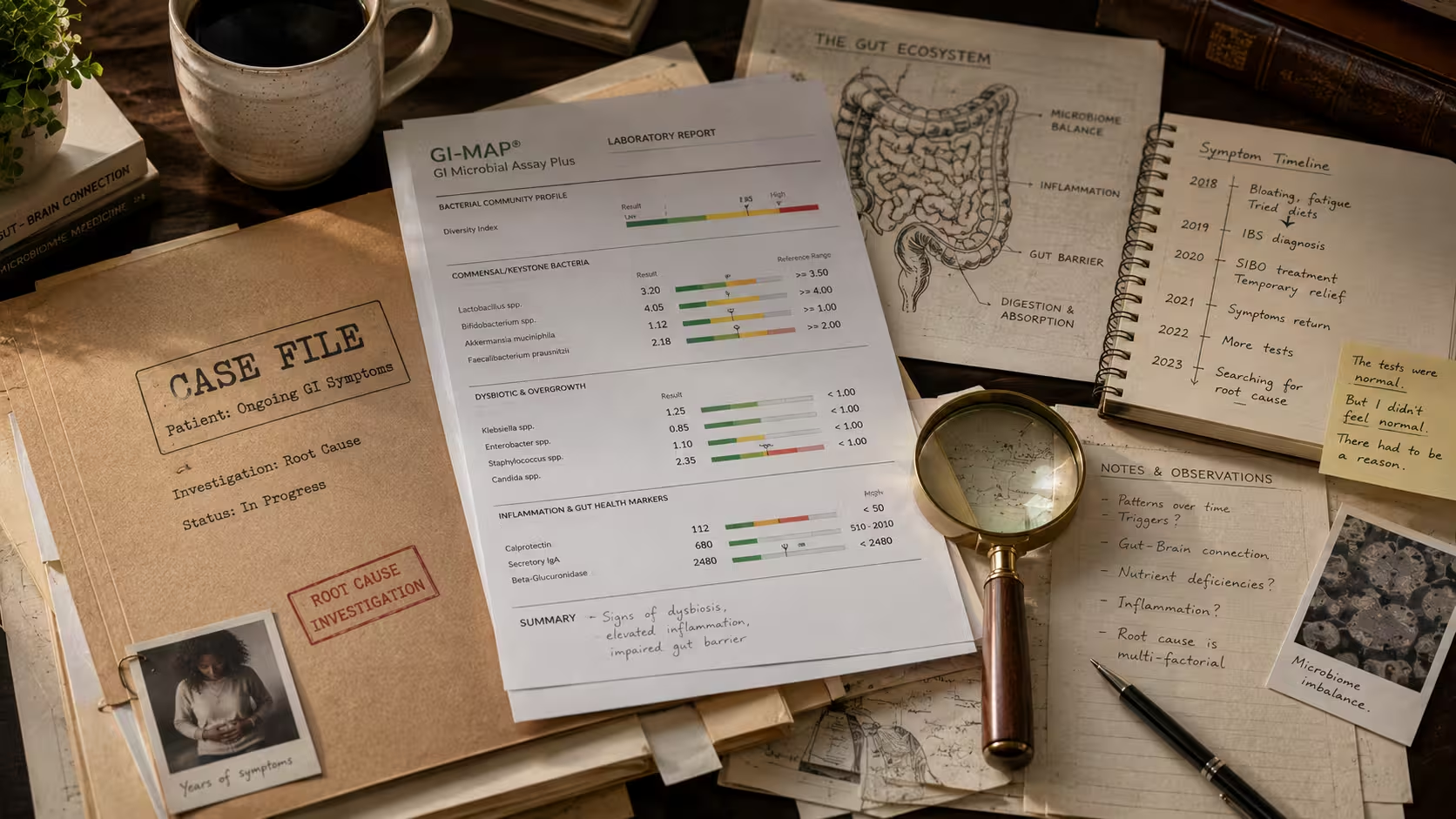
Marcus's GI-MAP Results: The Page That Explained 14 Years
When Marcus finally ran a GI-MAP through a functional medicine practitioner, the report didn't look anything like his old lab work. It wasn't a simple list of "normal" or "abnormal" flags, either. It was a picture of an entire ecosystem — and that ecosystem was clearly struggling.
Without turning this into a lecture, here's the shape of what showed up (all details anonymized):
- An H. pylori signal with virulence factors — the kind of finding a DNA-based test surfaces and a basic screen often misses. On its own, this is exactly what a DNA-based H. pylori stool test is built to catch, and it can drive bloating, reflux, and disrupted digestion.
- Bacterial overgrowth in the opportunistic category — classic gut dysbiosis, consistent with years of chronic bloating and gas.
- Low elastase — suggesting his body wasn't producing enough digestive enzymes to fully break down meals, which feeds bloating and starves the beneficial bacteria downstream.
- Elevated calprotectin — a marker pointing to low-grade gut inflammation, the kind his colonoscopy (a snapshot of structure, not biochemistry) was never built to catch.
None of these findings is exotic on its own. But together? They told a coherent story. A quiet H. pylori situation disrupting digestion. An imbalanced microbial community. Weak enzyme output. Simmering inflammation. A loop that kept feeding itself.
Here's the mechanism, in plain terms. When H. pylori and dysbiosis blunt stomach acid and enzyme production, food doesn't get broken down well. Poorly digested food ferments. It feeds the wrong bacteria and makes gas — there's your bloating. That imbalance irritates the gut lining. That's the inflammation the calprotectin flagged. Inflammation then impairs digestion and absorption further, and that's where the fatigue and brain fog creep in. Round and round, for 14 years.
None of that shows up on a "fine" report. All of it shows up on a GI-MAP test.
What GI-MAP Results Interpretation Actually Takes
Here's the part that's easy to get wrong: a GI-MAP test report is only as useful as the person reading it.
This isn't a test you order, skim, and self-treat from. Real GI-MAP results interpretation means connecting each finding back to your symptoms, history, diet, stress, and timeline. Then deciding what's actually relevant. A number on a page is just data. Context is what turns it into a direction.
A few reasons this matters:
- Not every finding needs action. Some flagged organisms are commensal or clinically insignificant for a given person. Chasing every marker is how people end up on fifteen supplements and more anxious than when they started.
- Sequence matters. Practitioners often think in terms of an order of operations — addressing something like an H. pylori load and digestive support before aggressively reseeding the microbiome. Doing things out of order can backfire.
- The test is a starting map, not a verdict. The GI-MAP shows you the terrain. It doesn't walk the whole journey for you.
This is exactly why the GI-MAP is a practitioner-ordered test rather than something you'd grab off a shelf. In the US, you'll typically work with a functional medicine provider, naturopathic doctor, or trained clinician — you can find one through the Institute for Functional Medicine directory. (The Institute for Functional Medicine) The test kit itself usually runs $350–$500 out of pocket, and many people can put HSA or FSA funds toward it. Some clinics fold the results review into the consultation itself.
For Marcus, that interpretation made all the difference between another confusing lab report and an actual plan. If you want to walk in ready for that conversation, our first-appointment checklist covers exactly what to bring.
IBS vs. Gut Infection: Why Your Label Might Not Be the Whole Story
Marcus spent over a decade believing he "had IBS." What the GI-MAP suggested is that IBS was the description — not the cause.
This distinction matters, so let's be precise. Irritable bowel syndrome is a real, recognized condition, and for many people an IBS diagnosis is accurate and appropriate exactly as given. But IBS is defined by symptoms, not a specific mechanism. That means it can also become a catch-all label for "we couldn't find anything on standard testing."
Functional medicine gut testing asks a simpler question about the root cause of digestive issues: is there an identifiable, testable driver underneath these symptoms that conventional workups never looked for? Sometimes there isn't. And sometimes — like in this case file — there's an H. pylori signal, dysbiosis, and inflammation that were there the whole time, just invisible to the tools being used.
The takeaway here isn't "IBS isn't real." It's this: you may have been given a symptom label. But if no one ever investigated the root cause of your digestive issues with the right tools, your story may not be finished yet. A comprehensive stool analysis is one way to check. our complete guide to functional medicine gut health
Is a GI-MAP Test Worth It? An Honest Look
Let's be balanced here, because you deserve straight talk, not a sales pitch.
A GI-MAP test may be worth exploring if:
- You have persistent, unexplained gut symptoms despite normal standard testing
- You've been labeled with IBS but never had DNA-based gut microbiome testing
- You're working with a practitioner who can actually interpret and act on the results
It may not be the right first step if:
- You have red-flag symptoms like blood in your stool, unexplained weight loss, or a severe or sudden change. Those need conventional medical evaluation first, not a functional test.
- You'd be ordering it with no plan for expert interpretation
- You're expecting one test to be a cure. It's a map, not a destination.
Functional stool testing isn't magic, and honestly, it isn't for everyone. Research into gut microbiome analysis is still evolving, and no single test tells you everything. (Clinical Gastroenterology and Hepatology (via PubMed)) What it can do, and what it did for Marcus, is turn a decade of "unexplained" into something specific, investigable, and finally actionable.
That shift — from mystery to map — is the whole point.
Key Takeaways
- "Normal" standard testing means the few things that test screened for weren't found — not that your gut is healthy
- Conventional stool tests rely on culturing (which misses organisms that won't grow) and screen a short pathogen list; the GI-MAP reads DNA instead
- Marcus's GI-MAP revealed an H. pylori signal, dysbiosis, low elastase, and elevated calprotectin — a self-feeding loop invisible to 14 years of "fine" reports
- The test is a map, not a verdict — expert interpretation is what makes it useful, which is why it's practitioner-ordered
- Budget roughly $350–$500 out of pocket for the kit; many people can use HSA/FSA funds
- Red-flag symptoms (bleeding, weight loss, sudden severe change) need conventional evaluation first
- An IBS label describes symptoms; it doesn't always mean the root cause was investigated
Frequently Asked Questions
What is a GI-MAP test?
How is a GI-MAP test different from a regular stool test?
What can a GI-MAP test detect?
How much does a GI-MAP test cost in the US?
Can I order a GI-MAP test myself?
How long do GI-MAP results take?
Does a GI-MAP test replace seeing my doctor?
The Word After "Fine"
Marcus started with one word: fine. Fourteen years of it.
What changed his direction wasn't a miracle or a magic supplement. It was a different question, paired with a test sensitive enough to actually answer it. The GI-MAP didn't invent his H. pylori, his dysbiosis, or his inflammation. Those were there the whole time. It just made them visible — so for the first time, someone could work with the real problem behind his digestive issues instead of managing around it.
If you take one thing from this case file, let it be this: "normal" isn't the same as "answered." A GI-MAP test won't be the right path for everyone, and it's never a substitute for proper medical care. But if you've been stuck in the loop Marcus knew so well, it might be worth asking your practitioner whether it's time to look deeper than the symptoms.
Your next step: If chronic gut symptoms have been dismissed as "just IBS," download our free Root Cause Gut Health Guide. It walks you through the questions to bring your practitioner, and shows how functional stool testing fits the bigger picture. Because you deserve more than fine.
Fact Checked By Dr. Prerana Suryavanshi, MD, MBBS
This medical analysis has been peer-reviewed and vetted by a credentialed practitioner to ensure diagnostic safety.

Written by Dr. Pooja, PharmD
Dr. Pooja didn't set out to write about gut health and hormones. She set out to become a pharmacist — learning how drugs move through the body, why they interact the way they do, and what it actually takes to prove a treatment works. That training is still the lens she writes through today.
View all articles by Dr. Pooja