Why Is My Hair Falling Out? 6 Hair Loss Causes in Women
Shedding more than usual? Learn the 6 most common hair loss causes in women — hormones, thyroid, low iron, stress — and how to find your root cause.
On this page Read more
- What Causes Hair Loss in Women? (The Quick Answer)
- First Things First: Normal Shedding vs. Real Hair Loss
- 1. Hormonal Hair Loss: The #1 Driver for Women
- 2. Nutritional Deficiencies: When "Normal" Labs Aren't Optimal
- 3. Stress and Telogen Effluvium: The 2-Month Delay Nobody Warns You About
- 4. Autoimmune Causes and Traction Alopecia
- 5. Genetics, Age, Thyroid, and Medications
- Why Female Hair Loss Is Rarely Just One Thing
- What Labs and Questions to Bring to Your Doctor
- Bonus: Seasonal Shedding and the Rosemary Oil Debate
- Key Takeaways
- Your Next Step
- Frequently Asked Questions
Reading time: ~9 min | Last reviewed: July 2026
You notice it in the shower drain first.
Then wrapped around your brush. Then on your pillow, in a cluster that makes your stomach drop. And suddenly, parting your hair — something you've done a thousand times without thinking — makes your heart sink.
If that sounds familiar, hear this first: you're not overreacting, and you're not alone.
More than half of all women experience noticeable hair loss at some point, according to the Cleveland Clinic. (Cleveland Clinic) By age 50, up to 40% of women have visible hair thinning, per UCLA Health. And yet female hair loss is still treated like a vanity problem — something to cover up, work around, or quietly accept.
This post takes a different approach.
The most powerful question isn't "How do I hide it?" It's "What's actually causing this?" Because here's the single most important thing to know about hair loss causes in women: the cause determines whether your hair grows back.
Let's find yours.
What Causes Hair Loss in Women? (The Quick Answer)
Hair loss in women is most often caused by hormonal shifts (menopause, PCOS, thyroid disorders, postpartum changes), nutritional deficiencies like low ferritin or vitamin D, stress-triggered shedding called telogen effluvium, autoimmune conditions, genetics, certain medications, and tension from tight hairstyles. Many women have two or more causes at once.
Breaking that down:
- Hormonal hair loss — menopause, perimenopause, PCOS, thyroid dysfunction, postpartum shifts
- Nutritional deficiencies — especially low iron (ferritin) and vitamin D
- Physical or emotional stress — the trigger behind telogen effluvium
- Autoimmune conditions — like alopecia areata
- Genetics — female-pattern hair loss (androgenetic alopecia)
- Mechanical and medication causes — tight hairstyles, certain prescriptions
And here's the catch most articles skip: hair thinning in women is rarely one clean cause. It's usually a stack. That's exactly why the miracle shampoo or the $60 biotin gummy doesn't deliver — you can't treat what you haven't identified.
Start there.
First Things First: Normal Shedding vs. Real Hair Loss
Before we go further, take a breath. Losing hair every single day is completely normal.
The American Academy of Dermatology says shedding 50 to 100 hairs per day is typical. (American Academy of Dermatology) Shedding noticeably more than that on a consistent basis — or noticing a widening part, a thinner ponytail, or distinct patches — is worth mentioning to a doctor. But the real question isn't how many hairs you're losing — it's whether they're growing back.
To see why, picture your hair on a three-phase cycle:
- Anagen (growth): Each follicle spends 2 to 7 years actively growing a hair. About 85–90% of your hair is here right now.
- Catagen (transition): A few weeks where the follicle shrinks and the hair detaches.
- Telogen (rest and release): The hair rests for a few months, then sheds to make room for a new one.
In a healthy scalp, follicles cycle out of sync — so you never notice.
Hair loss happens when something disrupts that rhythm. Either too many follicles hit the resting phase at once (a sudden shed), or follicles begin to miniaturize, so each new hair grows back thinner and shorter — until some stop growing at all.
Nearly every cause of female hair loss works through one of those two mechanisms. Knowing which one you're dealing with is half the battle.
1. Hormonal Hair Loss: The #1 Driver for Women
Hormones are the single biggest engine behind hair loss in women — and they shift at every predictable life stage.
Clues this is your category: thinning that tracks a life event (a baby, perimenopause, stopping birth control), a widening part, or hormonal company like irregular cycles, adult acne, or hot flashes.
Female-Pattern Hair Loss (Androgenetic Alopecia)
This is the most common type of female hair loss in the US, affecting an estimated 30 million American women, according to the Cleveland Clinic.
Unlike male-pattern baldness — which recedes at the temples — female-pattern hair loss shows up as diffuse thinning across the crown and a widening center part. Some dermatologists describe a "Christmas-tree" pattern when viewed from above.
It's partly genetic, and partly about how your follicles respond to androgens (hormones like testosterone). DermNet notes it can start as early as your teens or twenties, though it becomes far more common after menopause.
Menopause and Perimenopause: Hair Thinning in Women Over 40
As estrogen and progesterone decline through perimenopause and menopause, their protective effect on the hair cycle fades. Androgens — already present in your body — gain relative influence. The result is a slow, diffuse thinning that women often describe as their hair just... losing its fullness.
It's one of the most underdiagnosed forms of hormonal hair loss — and one of the least discussed.
PCOS and Androgen Excess
Polycystic ovary syndrome (PCOS) raises androgen levels — which is why PCOS hair loss usually travels with irregular periods, adult acne, or unwanted facial hair. The Androgen Excess and PCOS Society confirms the link between female-pattern hair loss and androgen excess. (Journal of Clinical Endocrinology & Metabolism (via PubMed))
This is a root cause worth ruling in or out — not just managing on the surface. If these symptoms sound familiar and your OB-GYN hasn't raised it, bring it up at your next appointment.
Postpartum Hair Loss
Losing alarming amounts of hair a few months after giving birth? You're likely experiencing telogen effluvium triggered by the postpartum hormone crash.
During pregnancy, high estrogen holds hairs in the growth phase. After delivery, that pause lifts — and months' worth of "on hold" hairs release at once. Postpartum hair loss typically peaks around month three or four and usually resolves on its own within a year.
It feels terrifying. It's almost always temporary.
The takeaway: when hair thinning in women tracks a hormonal life event, the timeline is your biggest diagnostic clue.
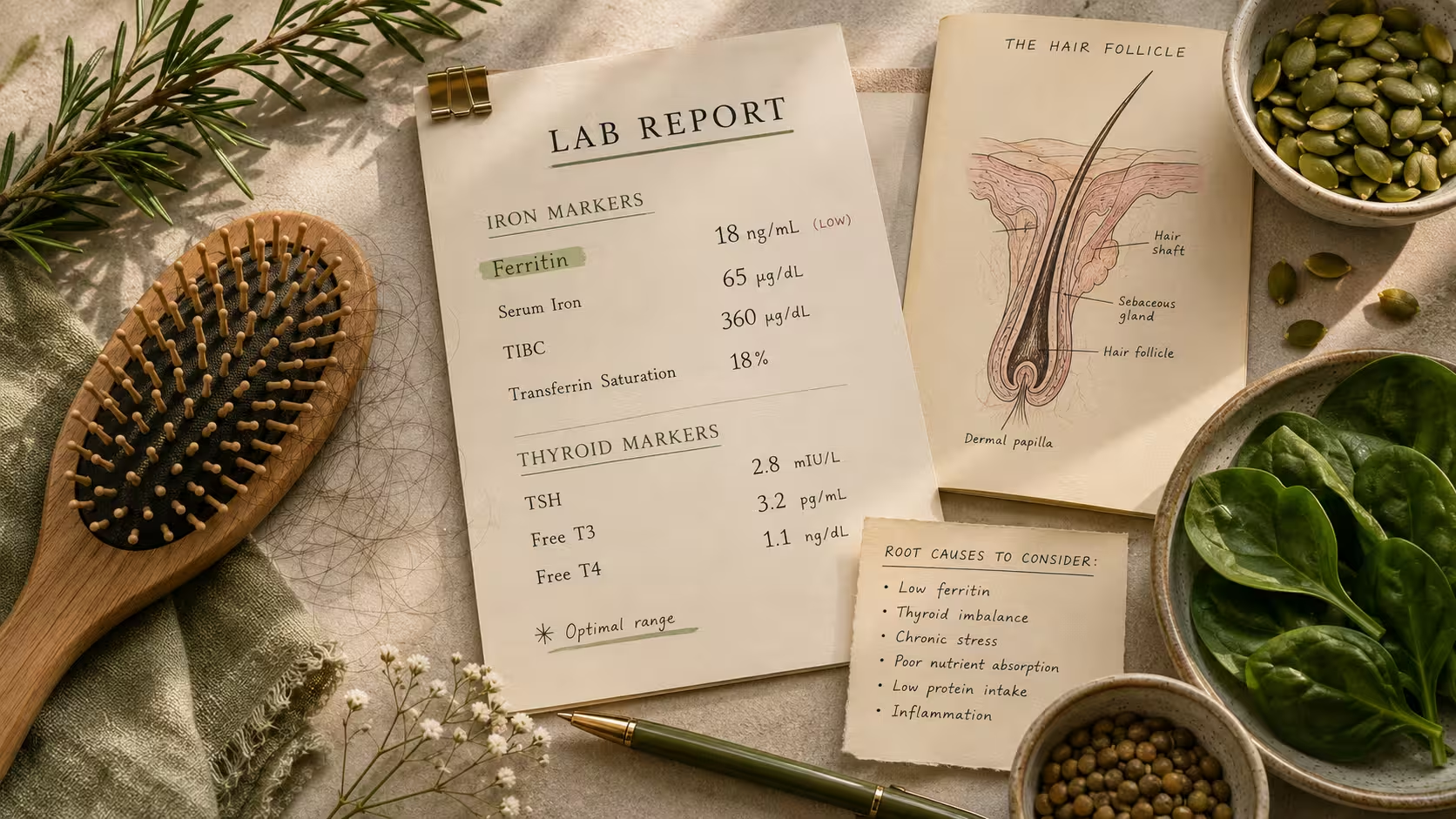
2. Nutritional Deficiencies: When "Normal" Labs Aren't Optimal
Your hair follicles are some of the most metabolically demanding tissue in your body. When a key nutrient runs low, hair growth is one of the first "non-essential" functions your body quietly deprioritizes.
Clues this is your category: heavy periods, a restrictive diet or recent rapid weight loss, fatigue, brittle nails, or labs that came back "fine" without anyone showing you the actual numbers.
Iron (ferritin). Low iron stores are one of the most overlooked hair loss causes in women — especially in the US, where standard lab reference ranges run notoriously wide. Here's the frustrating part: your ferritin can sit inside the "normal" range and still be far too low to support healthy hair growth.
Take a reader I'll call Ashley. Her ferritin came back at 14 — technically in range. She was told her bloodwork looked "fine." But hair-focused dermatologists and functional medicine practitioners typically look for considerably higher stores. Once Ashley and her doctor addressed her iron levels, her shedding slowed over the following months — and fine regrowth followed. Normal and optimal are not the same number, and for ferritin and hair loss, the gap between them matters enormously. normal vs. optimal lab ranges
Vitamin D. Vitamin D receptors participate directly in the hair cycle, and deficiency is remarkably common in the US — especially in northern states or for anyone spending most of the day indoors.
Zinc, B12, and protein. Crash diets, highly restrictive eating, and rapid weight loss can trigger significant shedding weeks later. Your body diverts scarce resources away from hair to protect essential functions first.
This is also why the $40 "hair, skin, and nails" gummy so rarely works. If you're not deficient in what's in the bottle, more of it changes nothing. And if you are deficient in something it doesn't contain, you've solved the wrong problem entirely.
3. Stress and Telogen Effluvium: The 2-Month Delay Nobody Warns You About
Telogen effluvium is the medical term for stress-related shedding — the driver behind that alarming "my hair is coming out in handfuls" experience.
Clues this is your category: sudden, diffuse shedding all over (not patches), starting two to three months after a major stressor.
Here's what's happening: a significant physical or emotional shock — surgery, high fever, illness, childbirth, a devastating breakup, financial crisis, crash dieting, or a prolonged stretch of intense stress — pushes a large share of your follicles into the resting phase at once.
Then, about two to three months later, all those hairs shed together.
That delayed timeline is why telogen effluvium gets missed so often. By the time hair is falling, the trigger feels like old news. You've moved on. Your follicles are just catching up.
The good news? Telogen effluvium is usually temporary. Once the trigger resolves, most women see shedding stabilize within three to six months, with regrowth behind it. The hard part is the waiting — and making sure a second cause isn't quietly running underneath. Chronic stress and the inflammation it drives can be exactly that kind of hidden second layer.
4. Autoimmune Causes and Traction Alopecia
Two categories of female hair loss look very different from diffuse thinning — and get missed because of it.
Alopecia areata is an autoimmune condition where the immune system mistakenly attacks healthy follicles, producing smooth, round bald patches rather than overall thinning. It can come and go, and that patchy pattern is the distinguishing sign.
Traction alopecia is mechanical: years of tight ponytails, braids, weaves, or extensions put constant tension on follicles — especially along the hairline — until they give out. The AAD notes this disproportionately affects Black women, along with scarring conditions like central centrifugal cicatricial alopecia (CCCA).
If you notice patchy loss or hairline recession specifically, don't wait. Scarring alopecias are time-sensitive — the sooner a board-certified dermatologist examines your scalp, the more can usually be preserved.
5. Genetics, Age, Thyroid, and Medications
Some hair loss causes in women come down to biology or the prescription list.
A family history of thinning on either side raises your odds of female-pattern loss significantly. Age gradually shortens the growth phase for everyone. Thyroid hair loss deserves special mention here: both an underactive and an overactive thyroid disrupt the hair cycle, and thyroid disorders overwhelmingly affect women.
Certain medications — including some used for blood pressure, mood disorders, thyroid conditions, or hormonal management — also list shedding as a side effect.
None of this means you're out of options. It means the honest first step is knowing what you're dealing with — before spending money on products that don't address it.
Why Female Hair Loss Is Rarely Just One Thing
Real life doesn't hand you a single tidy diagnosis. It hands you a stack.
A woman entering perimenopause may also have borderline-low ferritin and be running on five hours of sleep through a brutal season at work. Each factor alone might be manageable. Stacked together? They tip her past the threshold into visible thinning.
This is why chasing one miracle product almost always disappoints. Hair thinning in women is typically a systems problem — and it responds to a systems approach. Addressing the hormonal, nutritional, and stress drivers together produces results that treating any one alone simply can't.
What Labs and Questions to Bring to Your Doctor
You don't need to self-diagnose — that's what a board-certified dermatologist (or a trichologist, who specializes in hair and scalp health) is for. But you can walk in prepared.
Ask your doctor to look at:
- A full thyroid panel — not just TSH; ask about T3 and T4 too
- Ferritin specifically, not just hemoglobin — and ask about optimal ranges, not just "normal"
- Vitamin D levels
- Androgen markers (free and total testosterone, DHEA-S) — especially with irregular cycles or signs of androgen excess
- A scalp exam to distinguish diffuse thinning, patchy loss, or scarring patterns
Before your appointment, jot down: when you first noticed the shedding, any major life events in the prior three to four months, your family history, and any new medications or supplements. That context often points a good clinician to the cause faster than any single lab value.
If cost or coverage is a concern, community health centers and dermatology residency clinics often offer hair loss evaluations at reduced cost.
Bonus: Seasonal Shedding and the Rosemary Oil Debate
Two things worth knowing before you spiral down the internet rabbit hole.
Seasonal shedding is real. Research on healthy women found follicles enter the resting phase more in late summer — meaning the heaviest visible shedding often lands in September and October. Extra hair in the fall drain isn't automatically a red flag.
Rosemary oil: real science or TikTok hype? Somewhere in the middle. A 2015 trial in SKINmed compared rosemary oil to 2% minoxidil over six months and found comparable hair counts. (SKINmed (via PubMed)) That's what sparked billions of views. But it's one small study, essential oils can irritate the scalp, and product potency varies wildly. Rosemary oil is worth being curious about — it's not a substitute for finding your root cause. (Minoxidil, by contrast, is FDA-approved for female-pattern hair loss with decades of data — worth discussing with your dermatologist if genetics are in play.)
Key Takeaways
- Shedding 50–100 hairs a day is normal; a consistently wider part, patches, or noticeably heavier daily shedding is worth investigating
- The cause determines whether hair grows back — identify before you treat
- Hormones (menopause, PCOS, thyroid, postpartum) are the most common driver of hair loss in women
- "Normal" ferritin is not the same as optimal ferritin — ask for the actual number
- Stress-related shedding shows up two to three months after the trigger
- Patchy loss or hairline recession needs a dermatologist promptly — scarring types are time-sensitive
- Most women have more than one cause stacked — treat it as a systems problem
Your Next Step
That drop in your stomach when you saw your brush this morning? It's valid — not vanity, but your body signaling that something upstream deserves attention.
Almost every common cause of female hair loss is treatable once you identify it. So start by noticing the pattern. Diffuse thinning or a widening part? Distinct patches? Hairline changes? Did it follow a baby, a surgery, a hard stretch, or a new prescription? Document the timeline and bring it to a dermatologist or trichologist who focuses on hair loss.
Because the goal was never just to cover it up. The goal is to understand it.
Ready to walk into that appointment prepared? Download the free Female Hair Loss Root Cause Checklist — a one-page guide to track your symptoms, timeline, and lab gaps before your first visit.
Frequently Asked Questions
Why is my hair falling out so much all of a sudden?
What deficiency causes hair loss in women?
Can hormonal hair loss grow back?
Does menopause cause permanent hair loss?
How much hair loss per day is normal for a woman?
What kind of doctor should I see for female hair loss?
Female Hair Loss Root Cause Checklist
Download our free checklist to understand the root causes.
Download PDF FreeFact Checked By Dr. Prerana Suryavanshi, MD, MBBS
This medical analysis has been peer-reviewed and vetted by a credentialed practitioner to ensure diagnostic safety.

Written by Dr. Pooja, PharmD
Dr. Pooja didn't set out to write about gut health and hormones. She set out to become a pharmacist — learning how drugs move through the body, why they interact the way they do, and what it actually takes to prove a treatment works. That training is still the lens she writes through today.
View all articles by Dr. Pooja